
Imanuel Ross is the founder of Naturalistico, a platform dedicated to exploring holistic well-being and the human experience. He holds a Bachelor’s degree in Psychology and Counseling from the University of the Sunshine Coast, Australia. With a deep passion for understanding the human condition, Imanuel focuses on helping individuals achieve balance, self-awareness, and personal growth through natural and mindful approaches.
Polyvagal therapy evidence: what you can and can’t say to clients
Published on April 30, 2026
Polyvagal language is everywhere now—in session plans, websites, and the way many of us talk about safety and connection. With that visibility comes real pressure: clients ask whether breath or humming will “reset the vagus,” peers debate the physiology, and marketing can drift into promises no one can responsibly stand behind. The practical need is simple: speak clearly about state work, stay evidence-aware without sounding clinical, and keep consent and culture at the center.
Polyvagal theory offers a helpful map—especially when it’s used as a lens for building steadier states, stronger connection, and more choice in the moment. Traditional and ancestral regulation practices also offer deep, time-tested wisdom about rhythm, breath, sound, prayer, and community. When these two streams are held together with respect, the work becomes both grounded and human.
Key Takeaway: Use polyvagal language as a practical map for noticing states and supporting connection without promising specific physiological “resets.” Stay evidence-aware by focusing on observable shifts, consent-led pacing, and co-regulation, while honoring cultural and ancestral practices as complete traditions—not just biology.
What polyvagal theory actually says about safety, state, and connection
Put simply, polyvagal theory describes a few broad patterns the body uses to meet the world. Naming them helps clients recognize what’s happening inside—without pathologizing it—and understand why connection often becomes easier when safety is genuinely felt.
Hierarchy, neuroception, social engagement
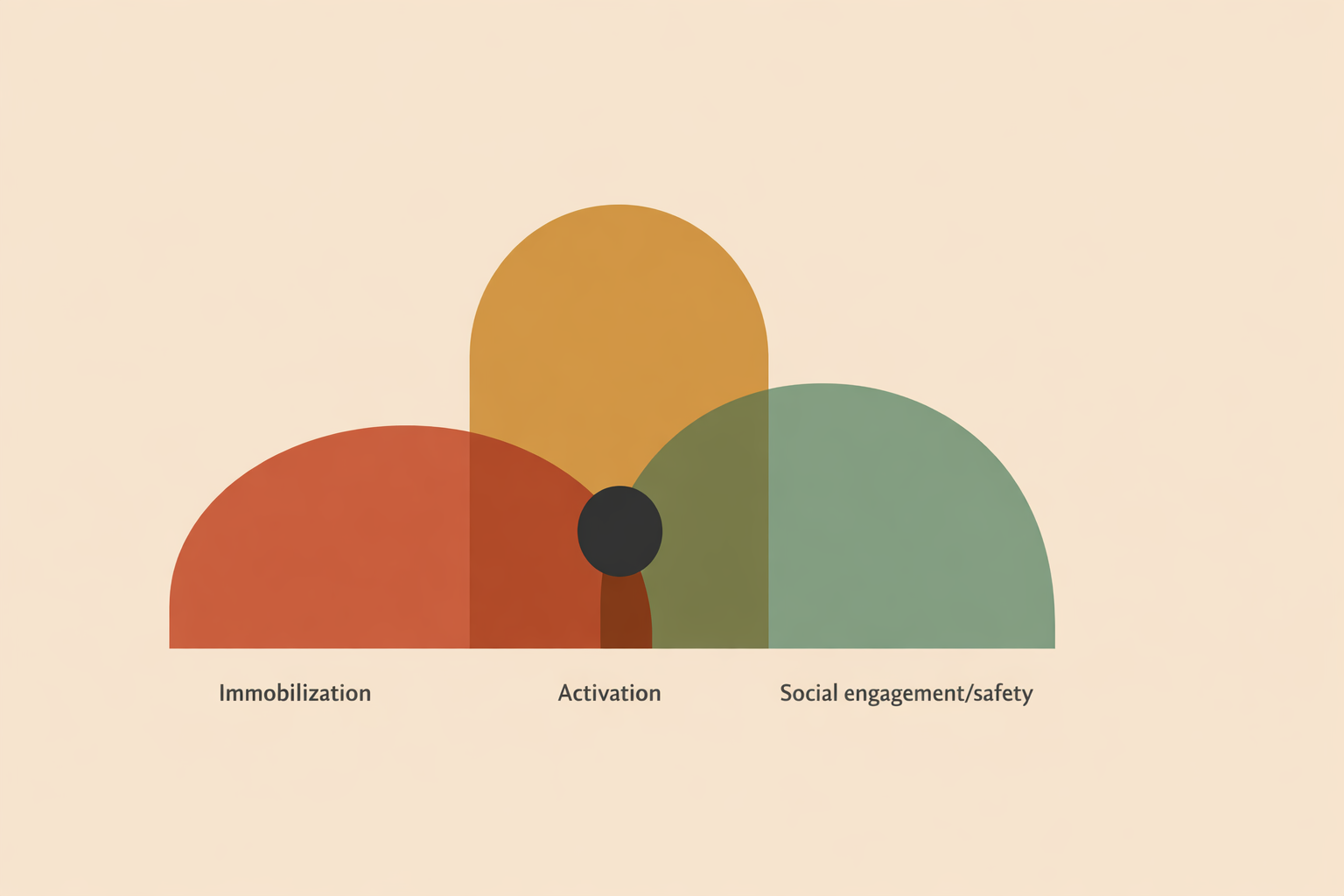
The framework highlights an unmyelinated dorsal vagal pathway (often linked with immobilization or collapse), the sympathetic system (fight/flight), and a myelinated ventral vagal system (social engagement). When ventral leads, people tend to orient, listen, and connect. When defense leads, they mobilize or shut down to protect themselves. Polyvagal theory also emphasizes a social engagement system that coordinates facial expression, vocalization, and listening.
Think of social engagement as the body’s “welcome signal.” It often shows up through facial expression and vocal prosody—the melody and tone of the voice. That’s one reason a steady voice, paced timing, and kind eye contact can be so regulating for many people.
Underneath it is neuroception, the ongoing (and often invisible) process of scanning for danger or safety. As Porges explains, the system must “assess risk” before it can ease out of defense and allow connection.
Through a polyvagal lens, our actions are “automatic and adaptive,” not moral failings or weak will.
When ventral support is present and safety is truly sensed, clients often find more room for experimentation. In Deb Dana’s words, that shift can open space for “curiosity and change.”
What you can confidently say: evidence‑aligned polyvagal benefits
You can speak confidently about building state awareness, supporting co-regulation, and practicing skills that often correlate with better flexibility under stress—especially when you focus on observable shifts and lived experience, not guaranteed biological outcomes.
Evidence-aligned ways to describe benefits
In psychophysiology research, autonomic flexibility (often discussed alongside “vagal tone”) is associated with positive emotions and social connectedness. Reviews also discuss how state shifts can show up in markers such as HRV and RSA. What this means is: there’s shared language for tracking change, without turning a complex human process into a single number.
Many commonly used practices—slow breathing, subtle movement, sound and humming, and a warm prosodic voice—are frequently linked in the literature with calmer emotions and improved self-regulation, and can support autonomic flexibility. Approaches like HRV biofeedback also point to meaningful benefits for some people, especially when the pacing is thoughtful and the relationship feels safe.
When you describe benefits, keep it practical and trackable:
- “We’ll build awareness of your states and practice shifting toward connection.”
- “We’ll use breath and sound to gently support your vagal system and widen your window of engagement.”
- “We’ll co-create signals of safety so your body has more room to settle and respond.”
As Porges notes, mindfulness “requires feeling safe.” That’s why tone, pacing, and presence aren’t “extras”—they’re often the doorway. Guidance for polyvagal-informed practice also emphasizes accessible ways to nurture vagal tone and state flexibility while staying away from medical-style promises.
What you shouldn’t promise: polyvagal claims beyond the evidence
Polyvagal work can be deeply useful in practice, but integrity comes from making claims you can stand behind. The simplest rule: avoid promising specific outcomes tied to specific nerve pathways, and be cautious with cause-and-effect language that the broader research base can’t yet confirm.
Phrases to retire or carefully reframe
Be careful with absolute statements that present the ventral vagus as a single “social engagement nerve,” or the dorsal vagus as a universal “shutdown switch.” A Medical Journal of Australia overview strongly critiques popularized assumptions and calls for more physiological precision in how people speak about pathways.
Some commentary describes certain applications as “scientifically questionable” yet still meaningful in lived practice—an invitation to hold the model as a working map rather than a final truth. Similarly, HRV and RSA are meaningful markers but are not straightforward readouts of one specific vagal branch. So it’s best not to promise that a single exercise will “increase ventral vagal tone” in a direct, guaranteed way.
Recent analyses also question simplistic stories about “freeze” and shutdown when the physiology isn’t clearly demonstrated. A cleaner approach is to name what’s observable—numbness, collapse, detachment, agitation—without overselling the circuitry.
Finally, polyvagal language is most responsible when presented as one lens among many, especially in multicultural and community work. That stance supports accuracy, flexibility, and respect.
Breath, sound, and bodywork: safety, risks, and consent
Breath, vocalization, rhythm, and touch can be profoundly regulating when paced well and grounded in consent. They can also overwhelm when intensity is pushed, context is missing, or the person’s signals are overridden. Skill here is less about “doing more” and more about titration—small steps that preserve choice.
Screening and pacing nervous-system practices
Screen gently. Strong breathwork can shift blood gases and contribute to respiratory alkalosis, which may feel like tingling, dizziness, tightness, or visual changes. Essentially, it’s a sign to adjust intensity, posture, and pacing—so the practice supports steadiness rather than triggering alarm.
Track shutdown and dissociation. “Spacing out” can be protective, especially with a history of overwhelm, and it often deserves respect rather than confrontation. Neurobiological writing on dissociation emphasizes grounding and relational pacing as supportive ways to reduce the risk of re-overwhelm. Look early for flattening, vagueness, sudden fatigue, or a sense of “gone,” then respond with warmth and smaller steps.
As Deb Dana writes about collapse, sometimes we try to “become invisible” to survive.
Meet that with steadiness, not pressure. Keep options open and let the person decide what “enough for today” looks like.
Practical guardrails:
- Pre-check: Ask about dizziness history, panic, fainting, or sensitivities to sound/touch. Offer seated or lying options from the start.
- Consent in layers: “We can stop anytime. You choose the pace, the volume, and whether touch is included.” Keep checking in.
- Go from gentle to strong: Begin with nasal breathing, longer exhales, soft humming, or swaying before any stronger practices.
- Watch the window: If there is rapid breathing, numbing, or overwhelm, pause, orient to the room, and return to simple cues of connection.
- Red flags: Chest pain, fainting, or intense emotional flooding—stop, ground, and reassess whether today is the right time for further activation.
Bringing in ancestral regulation wisdom without over‑claiming
Across cultures, rhythm, breath, song, prayer, and community have supported steadiness for centuries. Polyvagal language can complement that wisdom by describing how co-presence and rhythm may help the body sense safety—without shrinking rich traditions into biology alone.
Honoring rhythm, breath, and song across cultures
Many traditions use rhythmic breathing, chanting, and gentle movement to soothe and connect, held within story, ritual, and belonging. Contemporary somatic and mindfulness research echoes parts of this picture, linking some practices with HRV shifts and increases in autonomic flexibility.
In practice, invite what is authentic to the client. Ask what rhythms, songs, prayers, or community practices belong to their lineage and feel genuinely supportive now. Let them lead the language and boundaries. If polyvagal explanations help them feel less shame or more agency, use them; if not, the tradition can stand on its own.
Community matters here. Relational perspectives emphasize that felt safety is social, and people engage more freely when relationships and environments feel trustworthy. Research also suggests that social connectedness and regulation often strengthen together over time.
Equity-focused resources connect polyvagal ideas with belonging and social context, reminding us that safety is shaped by culture, environment, and power—not just individual mindset. One reflection describes polyvagal work as “the science of feeling safe enough to fall in love with life,” which captures the heart of why this language resonates.
Turning polyvagal evidence into ethical scripts for sessions and marketing
Warm, clear language builds trust. These ready-to-use phrases keep agency central, stay aligned with evidence, and communicate polyvagal ideas without hype.
From hype to honest, grounded language
Set the frame (intake):
- “We’ll use a polyvagal lens as one way to notice your body’s signals and practice steadier states. It’s not the only lens, and you’re the expert on what works for you.”
- “I’ll offer options like breath, sound, and gentle movement. You choose what feels supportive, and we’ll stop or adapt anytime.”
Explain the why (early sessions):
- “Your nervous system constantly scans for safety—that’s normal and protective. When more safety is sensed, connection often gets easier.”
- “We can build cues of safety together—voice tone, eye contact, paced breath—so your body can settle before we go deeper.”
Teach state mapping (coaching moment):
- “Let’s name today’s state—connected, revved, or collapsed—so we can match a practice to it.”
- “Notice what helps you feel anchored. As Deb Dana says, find something that reminds you of being ‘anchored’ and keep it nearby.”
Offer practices without over-claiming:
- “Longer exhales and soft humming can support vagal flexibility and calmer feelings. We’ll go slowly and see what your body prefers.”
- “We’ll watch for markers like easier breath, warmer hands, or clearer focus—your lived signals matter more than any gadget.”
Co-regulation language (relational safety):
- “I’ll keep my voice soft and steady; if anything feels too much, say so and we’ll pause.”
- “When we don’t feel safe, we’re often in evaluation and defense,” as Porges notes—naming that can reduce shame about reactions.
Marketing copy (ethical, hopeful):
- “Polyvagal‑informed coaching to build safety, steadiness, and connection—through breath, rhythm, and relationship.”
- “Evidence‑aware practices to increase state flexibility (often reflected in HRV and RSA) and help you feel more at home in your body.”
Plain-language principle: Keep it simple and collaborative. Many practitioners point to Deb Dana for translating polyvagal theory into plain language. Similarly, coaching-aligned guidance emphasizes a collaborative framework: invite, don’t impose; describe, don’t dictate.
Conclusion: using polyvagal evidence wisely in what you say
Polyvagal-informed work offers a living language for safety and connection. When that language is paired with ancestral wisdom and current research—without reducing either—your message becomes a steady bridge: clear, respectful, and empowering.
Practically, that means promising state awareness and co-created safety rather than guaranteed outcomes. It means choosing gentle-first practices, pacing them carefully, and making consent the structure that holds everything. It also means treating HRV and RSA as useful context, not as the whole story—because the most meaningful measure is still the person’s day-to-day sense of steadiness, connection, and choice.
As the field refines its physiology, it’s wise to hold the model lightly and your care firmly. Present polyvagal theory as one lens that integrates beautifully with relational, somatic, and cultural practices you already trust. When warmth and accuracy travel together, trust grows without hype—and your work keeps evolving without losing its heart.
Published April 30, 2026
Train in polyvagal practice
Deepen your evidence-aware, consent-led language in the Polyvagal Therapy Certification.
Explore the Certification →
![]() Related courses
Related courses
Related courses

Efficientcoach
12 modules
Positive Psychology Coach Certification

Efficientcoach
11 modules
Art Life Coach Certification

Efficientcoach
12 modules
Grief Coach Certification

Efficient Therapist
11 modules
Play Therapy Certification

Efficientcoach
23 modules
Life Coaching Certification

Naturalistico
11 modules
Sex Therapy Practitioner Certification